How DNA Could Make Blood Donations a Thing of The Past
Made in collaboration with Alex A., Milind Kumar, Kevin Joseph, and Lior Rozin
There are a lot of things, medically speaking, that we don’t do anymore. We don’t cover people with donkey dung to ward off evil spirits. We don’t give children morphine to “help” with teething. We don’t drink mercury to increase our “vitality”.
Despite that, there is one medical practice that sounds just as ridiculous but is still in use today. It’s called blood transfusions. When someone has lost a lot of blood, doctors will take a bag of blood that another person has “donated” and stick it into the patient to replace the blood that they’ve lost. Sure, the procedure’s evolved a bit since the 1600s. We don’t use sheep blood anymore, and all the donors are willing participants. It just feels like there must be a better, 21st-century solution.
Why Blood Is Complicated
We all know that blood is important. Blood carries nutrients, gets rid of waste, and most importantly, carries the oxygen you need to stay alive. Our body’s supposed to produce blood on its own, but if you’ve been hurt or have certain conditions, you might need to “borrow” some from someone else.
Like anything involving humans, blood donations are complicated. In the US alone, someone is in need of life-saving blood every 2 seconds. The thing is, only 5% of the 40% of people who are eligible to donate do so.
There are two big problems there. First, there’s that 40% figure. Only just under half of Americans are eligible to donate blood. 22.1% of Americans are under 18, so I’ll exclude them from the remaining 60%. Even then, only 51% of US adults are eligible to donate blood.

The thing is, it’s really hard to raise this number any further. People can be ineligible to donate for a variety of reasons, encompassing everything from medical conditions (like certain cancers) to bloodborne diseases like HIV/AIDS and Hepatitis. All of these issues are different and each requires different solutions to mitigate.
There are also a bunch of reasons why that 51% of adults might choose not to donate blood. These reasons can be anything from a fear of needles to just not wanting to suffer the inconvenience of the donation process. Regardless of the reasons, more and more people are choosing not to donate blood each year. This is very bad. Someone is constantly in need of life-saving blood, and that blood is running out.
At the time of writing, the Canadian Blood Services only has a two days supply of B- blood. It also only has a three days supply of O- blood, the universal blood type. We aren’t trying to fearmonger here, but the situation isn’t great. Our system relies on the generosity of donors to give the blood needed to save others’ lives. If this generosity faltered for even a couple of days, the consequences can be disastrous.

To make matters worse, it isn’t like the blood banks can build up a stockpile of blood for emergencies (not that they have the supply for that, anyway). Donated blood only lasts 42 days before they have to throw it out, making building up any significant stockpile almost impossible.
When we really look at it, all these problems stem from the same source. Blood isn’t available because people are complicated and collecting blood from people is hard. Blood doesn’t last long because it comes from humans and isn’t meant to stick around outside the body. Even the eligibility problem can be traced back to humans. Humans get infections and these infections can prevent them from donating blood. But what if we could cut out the human?
Why We Don’t Have Artificial Blood (Yet)
We aren’t the first people to try to make artificial blood. On the face of it, synthetic blood should be extremely easy to make. You just need a substance that picks up oxygen in the lungs and drops it off in the tissues. Historically, oxygen-carrying blood substitutes attempted this using hemoglobin or perfluorocarbon emulsions to carry oxygen in the blood.
Perfluorocarbon Emulsions
Perfluorocarbon-based blood substitutes use perfluorocarbons to carry oxygen throughout the body. Because these chemicals aren’t water-soluble, they need to be turned into microscopic droplets to travel through the blood. Because of the small size of these droplets (smaller than red blood cells), they can theoretically get into small spaces that red blood cells can’t and deliver blood through blocked capillaries.
This solution isn’t as great as it first appears, though. While a perfluorocarbon-based blood substitute (Fluosol) was approved in 1989, it was taken off the market because of a number of issues. For one thing, patients using Fluosol had to “load” the substitute by breathing in pure oxygen. Fluosol also had a low half-life in the body (13 hours), meaning that it couldn’t replace biological blood in blood transfusions. Fluosol’s final nail in the coffin was the difficulty of storing it, leading to it being taken off the market in 1994.
Hemoglobin-Based Oxygen Carriers (HBOCs)
Your red blood cells are packed with a molecule called hemoglobin that they use to carry oxygen to your cells. Many companies thought, “if you don’t have enough red blood cells, why not just use pure hemoglobin?”
Unfortunately, hemoglobin is somewhat toxic in the body. Unmodified hemoglobin has a very high oxygen affinity that prevents it from properly carrying oxygen on its own. Hemoglobin also breaks down into smaller fragments (dimers) that can damage the kidneys and can cause toxicity. Finally, cell-free hemoglobin can take up nitric oxide in the blood vessels, causing high blood pressure (to a dangerous extent).
There are a bunch of companies that tried to make HBOCs, but all of them failed due to either running out of funding or the toxicity of their product. Take Biopure, for instance. Biopure used bovine hemoglobin to make their synthetic blood substitute. They had both a human version (Hemopure) and a veterinary version (Oxyglobin), but the human version was never approved in the US or UK due to safety concerns.
While these HBOCs also had the advantage of being able to pass through blocked blood vessels, their short half-life (19 hours for Hemopure) and side effects stop them from being the silver bullet we wish they could be. If you look at the companies that worked on HBOCs, you’ll find that they either ran out of money before completing clinical trials or shut down after safety concerns in their later trials. Biopure suffered this second fate, shutting down after the FDA raised concerns about the safety of their product (there were some legal issues too, read more here).
A Third Option
When we look at current blood substitutes, we see two bad options. We have perfluorocarbon emulsions, which have some benefits but aren’t effective enough to replace real blood. We also have hemoglobin-based oxygen carriers, which are better at carrying oxygen but have toxicity issues and a short half-life. Where can we go from here?
This is where Oxalis enters the picture. We looked at the issues with the current blood donation system and the problems with current solutions and decided to create a new solution that falls into its own, unique category. Instead of using synthetic chemicals or proteins to transport oxygen, we’re using DNA.
Aptamer-Based Oxygen Transport
When most people think of DNA, they think of it as a way to store information in cells. While this is one of its roles, DNA can do so much more that we’re only starting to explore.
If you think back to high school biology, you’ll remember that DNA is made up of complementary bases. Adenosine (A) binds to Thymine (T) and Cytosine (C) binds to Guanine (G).
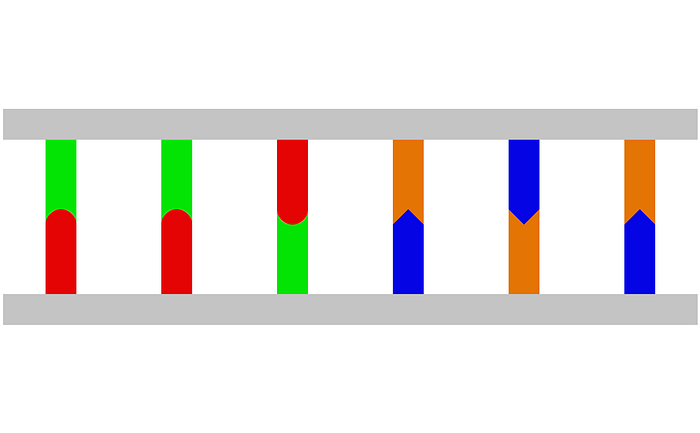
When DNA is storing information, it’s (generally) double-stranded DNA (dsDNA). Double-stranded DNA consists of two complementary strands of DNA that bind to each other, like in the above image.
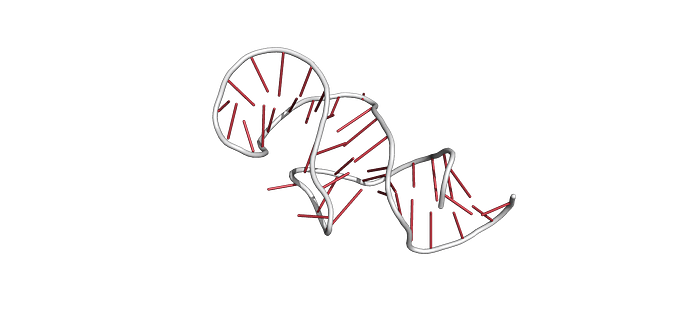
Double-stranded DNA can store information, but single-stranded DNA can do so much more. When you only have a single strand of DNA, the DNA will bend and twist itself to maximize the number of bonded complementary bases. The bases that aren’t bonded stick out and can bind to molecules or proteins around the DNA tangle.
We’re going to be focusing on a specific type of DNA tangle called an aptamer.
Think of aptamers like puzzle pieces. The tangle of DNA (see the image below) has a specific shape that fits with a specific molecule like a puzzle piece. If we had a “puzzle piece” that connects with oxygen, maybe we could fix some of the problems with HBOCs.
Directed Evolution
Okay, so we want to create an aptamer to transport oxygen. But how? Even small DNA sequences can have millions of variations, and it isn’t like we can test each one individually.
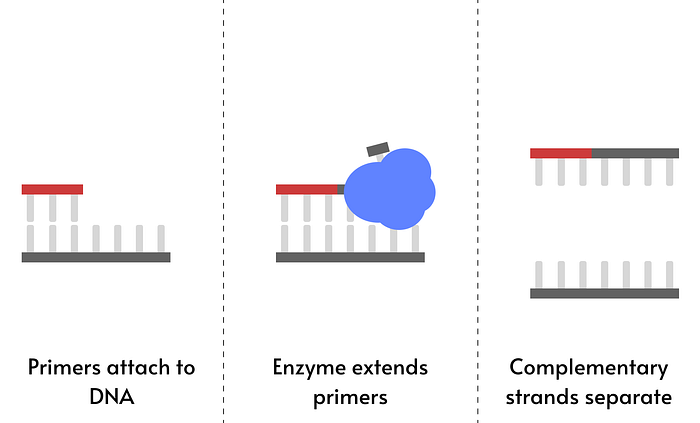
Luckily, there is a way that we can test millions of aptamers at the same time. In nature, evolution slowly makes better and better versions of a gene or protein, without trying out each and every possible variation. We can mimic this using a technique called directed evolution.
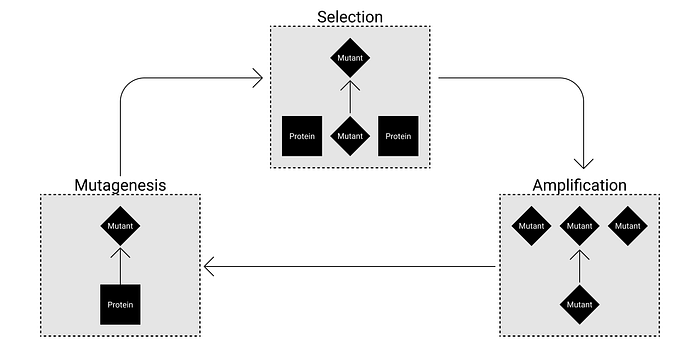
First, we need to create variation. We’ll start with a bunch of variants of a known aptamer that binds to heme (the molecule hemoglobin uses to transport oxygen) but doesn’t transport oxygen on its own.
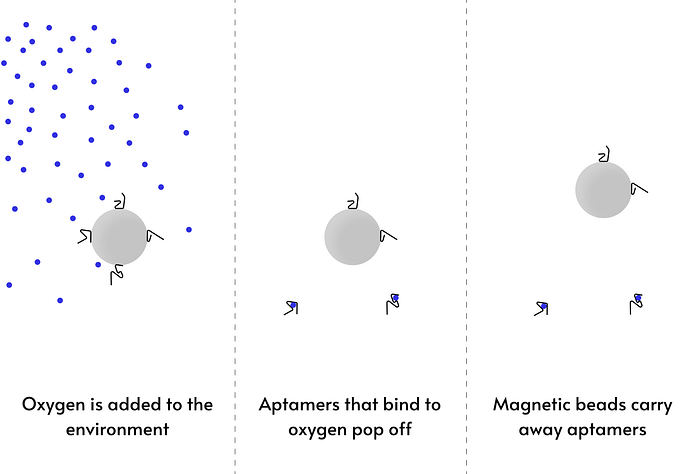
Next, we need to select for aptamers that carry oxygen. We’ll do this using a technique called structure switching SELEX. In this technique, we add a sequence to the aptamers that sticks to a special magnetic bead. If the aptamers bind to oxygen, their structure will change and they’ll pop off the bead. We can use this to select for aptamers that bind to and release oxygen. Once we have candidates, we can use spectral analysis to evaluate the hundreds of potential aptamers generated and pick out the best one.
We’ll also want to make sure our aptamer isn’t toxic. HBOCs can cause high blood pressure by binding to nitric oxide that’s keeping blood vessels open. We’ll add another step that uses structure switching to eliminate any aptamers that bind to nitric oxide.
Finally, we need to replicate the aptamers that survived this process. We’ll use normal PCR (think of COVID tests) to make exact copies of these aptamers alongside error-prone PCR to make variants of these aptamers. Each time we repeat this process, we’ll get aptamers that are better and better at carrying oxygen. However, we’ll eventually reach a point of diminishing returns where we have to test each aptamer on its own.
Protecting the Aptamer From The Body
Your immune system doesn’t like viruses. Because of this, it has a bunch of enzymes that it uses to get rid of free-floating DNA in your bloodstream. If we injected an unmodified aptamer into the bloodstream, it would be completely destroyed in minutes.
That’s a problem if we want to replace red blood cells. Red blood cells can last 120 days, so our solution needs to last more than a couple of minutes for it to be useful. Luckily, scientists have developed a version of RNA that can’t be degraded by enzymes in the blood. This synthetic nucleotide is called locked nucleic acid (LNA) and is resistant to the enzymes found in the blood. If we replace all the bonded nucleotides with LNA, our aptamer could last for a couple of days with no change in its activity.
A couple of days is better than the hours given by other methods, but it still isn’t good enough to replace red blood cells. Luckily, there’s another method that can be used with LNA to give us even longer lifetimes. Through a process called PEGylation, we can attach a polyethylene glycol subunit to the aptamer, letting it stay in the body longer. One study found that PEGylation in combination with LNA gave an aptamer a half-life of two weeks in the body. Of course, it would be great if the aptamer could last longer in the body. There are many ways we might be able to do this, for example by making the aptamers form dimers to decrease kidney filtration. Even if we can’t increase the half-life, two weeks is a long enough half-life to not require constant transfusions.
One final benefit of using aptamers is their ease of storage. Our aptamer can be dried and stored at room temperature indefinitely. Even if it wasn’t stored in optimal conditions, the aptamers could theoretically survive for up to 25 weeks at 37 degrees if dried. This is an incredible improvement over conventional blood, which can’t even survive 25 weeks when refrigerated.

So What?
Our goal with Oxalis is to create a solution to help healthcare professionals do what they do best — save lives. While our solution is somewhat unstable, it addresses most of the problems with regular blood and existing synthetic blood substitutes.
With that said, there are still a few challenges that we have to address. By far the biggest challenge we face is the scale of DNA synthesis required to make our aptamer. Because LNA is synthetic, you can’t replicate the aptamer using PCR. Instead, we have to synthesize the DNA one nucleotide at a time. After doing the math, we need a maximum of 150 grams of the aptamer to replace one unit of blood.
When it comes to conventional DNA synthesis, you’re probably looking to synthesize less than a milligram. Our solution requires 150 000 times that! And this is to replace one unit of blood (about a pint). If we replaced only 10% of the annual blood supply, we’d need to synthesize over 1300 metric tonnes of DNA and LNA per year. With that said, here is our worst, medium, and best case prediction for feasibility.
Worst case scenario, DNA and LNA synthesis can’t be scaled up any further. At this price point, our aptamer would cost about the same as blood to produce ($200-300). It wouldn’t be able to replace regular blood, but it could play a role in emergency situations by replacing blood types like O- that are in highest demand (since our aptamer wouldn’t have a blood type, it could be a substitute for anyone). This more expensive blood could also be a treatment for people with ultra-rare blood types, where very few people are able to give them blood.
Medium case scenario, DNA and LNA synthesis can be scaled up somewhat, and we can produce the blood at a price of $100-150. At this price point, our aptamer could completely replace the use of O- blood in emergencies where the patient’s blood type is unknown. It could also replace blood transfusions where the patient will regenerate quickly enough for the short half-life not to be a problem. However, natural blood transfusions would still be used when the patient is unable to regenerate their blood quickly and needs longer-lasting blood.
Best case scenario, a new type of PCR is created that can work with DNA and LNA. There is reason to believe this is possible since some variations of the enzymes used in PCR are able to unreliably incorporate LNA. It is possible that someone could create a variant of one of these enzymes that exclusively works with LNA, allowing us to replicate an aptamer using PCR. If this happened, our aptamer-based blood could completely replace natural blood. PCR reactions cost about $1.50 to double the DNA. Even if the LNA reagents were many times more expensive, we could still synthesize a unit of blood for well under $10 (minimum 20x reduction in cost).
As one of the people working on this, I‘m optimistic that option 3 will be true. If we could replicate our aptamer using PCR, the only thing we’d have to worry about would be the drug approval process. Existing synthetic blood substitutes have been given compassionate use authorization to treat people who can’t receive blood transfusions. Since our aptamer should have fewer side effects while lasting longer in the body, Oxalis should also be able to get this. Being given compassionate use authorization would allow us to help people with our aptamer while going through the full approval process.
Regardless of what happens with scaling and approval, I believe Oxalis will play a role in the blood ecosystem moving forward. While our solution only carries oxygen and doesn’t help with all the different jobs blood has to play, it was never meant to completely replace natural blood. Our solution is designed to keep people alive and healthy long enough for their bodies to take over and regenerate on their own.
A Quick Recap
So, as a quick recap, we want to help medical professionals save lives. To do this, we plan to:
- Evolve an aptamer that can carry oxygen without poisoning you
- Make a version of that aptamer that can last long in the body
- Use the expensive (first) version of that aptamer in specific situations where natural blood can’t be used
- Scale-up production to make the aptamer as inexpensive as possible to reduce the strain on our healthcare system
If this article piqued your interest in Oxalis and you’d like to learn more, check out our website at oxalismed.com.
